Get in touch: +1 888 453 5021





A medical resident is an MD graduate who participates in an Accreditation Council for Graduate Medical Education (ACGME)-accredited post-graduate training program.
Medical residents spend their first year of training as interns, also called PGY-1 residents. During this year, they work in hospitals, clinics, and specialty services under close supervision from senior residents and attending physicians. Interns are doctors, but they are still early in their clinical training, so their responsibilities are closely monitored.
After the intern year, residents usually gain more independence in three main areas:
Graduate Medical Education (GME) programs allow students to practice medicine on real patients. The goal is to bridge the gap between students and doctors with exposure to everyday life as a medical professional.
The terms medical intern, medical resident, and attending physician refer to different stages of a doctor’s training and career. An intern is a first-year resident, also called a PGY-1. Interns have graduated from medical school and earned their MD or DO degree, but they’re still at the beginning of their supervised clinical training.
A medical resident is a physician completing specialty training after medical school. Residents are grouped by postgraduate year (PGY-1, PGY-2, or PGY-3) based on their residency stage. During this time, they:
An attending physician has completed residency and, if applicable, fellowship training. Attendings are fully licensed physicians who can practice independently, supervise residents and interns, make final clinical decisions, and often lead patient care teams. In simple terms, interns are first-year residents, residents are doctors in specialty training, and attendings are fully trained physicians who oversee care.
Medical residents are responsible for the following tasks:
In hospital-based specialties, they may also:
In outpatient settings, they may:
Residents also spend a large part of their training learning from senior physicians. They work under the supervision of attending physicians, who review their decisions and guide patient care.
As residents advance from PGY-1 to later training years, they usually assume greater responsibility. Senior residents are usually responsible for:
In addition to clinical work, residents are expected to attend:
Many also participate in research, quality improvement projects, teaching, and board exam preparation.
Residency is designed to help doctors move from medical school knowledge to independent clinical practice.
To become a medical resident, you first have to complete medical school and earn a medical degree, either an MD or a DO. During medical school, students build the academic and clinical foundation needed for residency by completing classroom coursework, clinical rotations, board exams, and specialty exploration.
Most medical students begin preparing for residency well before graduation. This includes:
For many U.S. residency programs, applicants apply through the Electronic Residency Application Service (ERAS), where they submit materials such as:
After submitting applications, students may be invited to interview with residency programs. These interviews help programs assess an applicant’s:
If you need help preparing for your residency interviews, check out the video below:
Applicants then rank the best residency programs they interviewed at, while programs rank the applicants they would like to train.
Most applicants are placed into residency through the Match, a system that pairs applicants and residency programs based on both sides’ rank lists. Once matched, the applicant begins residency after medical school graduation, usually as a PGY-1 (intern).
From there, they complete several years of supervised specialty training before becoming eligible for independent practice or fellowship training.
Medical residencies typically last three to seven years, depending on the specialty. Some of the least competitive residencies, like Family Medicine, are very short, while other programs are very long. Some specialties are more competitive and may take longer due to limited availability.
We collected this data from the AMA’s Medical Specialty Training Length article.
You can find medical residencies by researching accredited programs in your chosen specialty and comparing them based on:
Most applicants start their search by identifying their specialty and then building a balanced list of programs where their academic profile, clinical experiences, and long-term goals align.
A good starting point is to use residency search tools such as the Fellowship and Residency Electronic Interactive Database Access (FREIDA), program websites, specialty society directories, and your medical school’s advising resources.
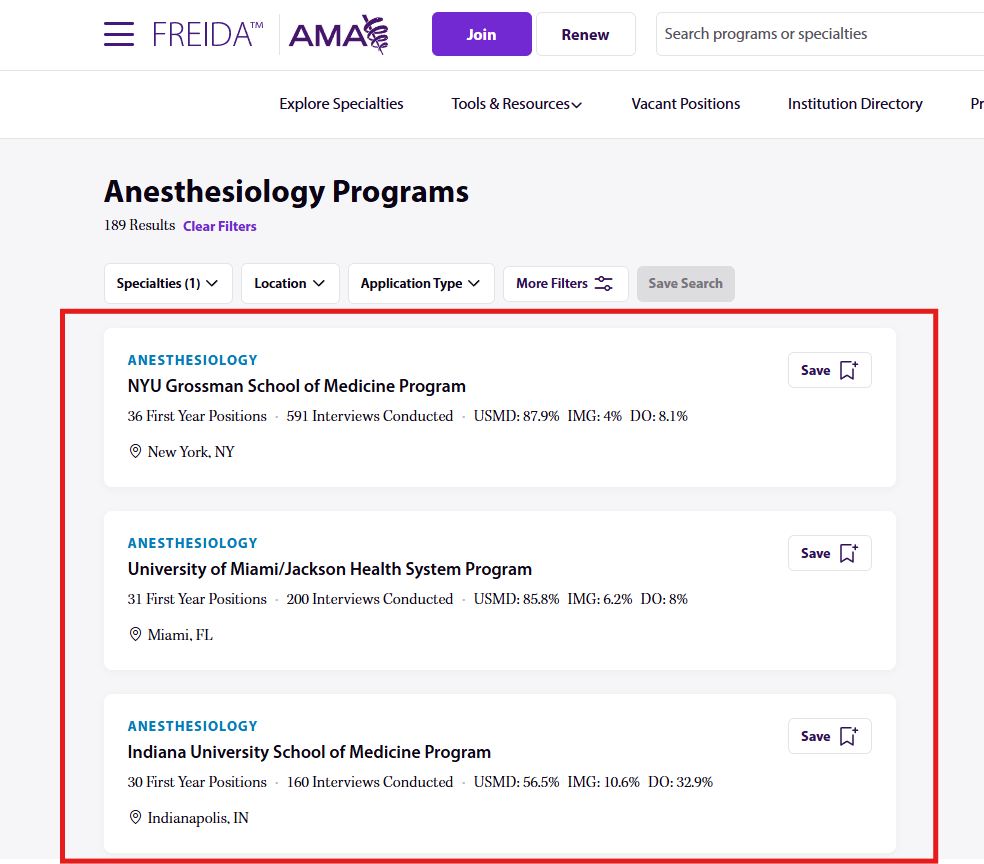
These sources can help you compare program details such as:
You can also find residencies through clinical rotations, away rotations, faculty mentors, alumni, residents, and specialty interest groups.
Speaking with people who know the program firsthand can give you insight into the culture, workload, mentorship, teaching quality, and residents' sense of support.
For personalized assistance with your residency application process, get residency application help from Inspira Advantage. Work with an expert residency advisor to help you choose the perfect program and get accepted.
The average U.S. medical resident salary in 2026 is $272,959. Here’s a look at the yearly salaries of medical residents from different states in the U.S.:
Medical residents often work long and demanding schedules, but their hours are regulated by the Accreditation Council for Graduate Medical Education (ACGME). In most U.S. residency programs, residents can work up to 80 hours per week, averaged over a four-week period. This includes:
Resident work hours vary by specialty, rotation, and year of training. A resident on an inpatient surgery, ICU, emergency medicine, or obstetrics rotation may have longer shifts, overnight call, or weekend coverage. A resident on an outpatient clinic, elective, research block, or lighter specialty rotation may have a more predictable schedule.
ACGME rules also require residents to have at least one day free from clinical work and required education every seven days, averaged over four weeks. In-house calls generally cannot be scheduled more often than every third night. And night float still has to fit within the 80-hour weekly limit.
For applicants, this means residency is closer to a full-time training program with a clinical apprenticeship than to a traditional 40-hour workweek. The exact schedule depends heavily on the program and specialty, but residents should expect early mornings, late nights, weekends, call shifts, and periods of high clinical responsibility throughout training.
After completing residency, physicians can move from supervised specialty training into the next stage of their medical career. For many doctors, this means becoming an attending physician, where they can:
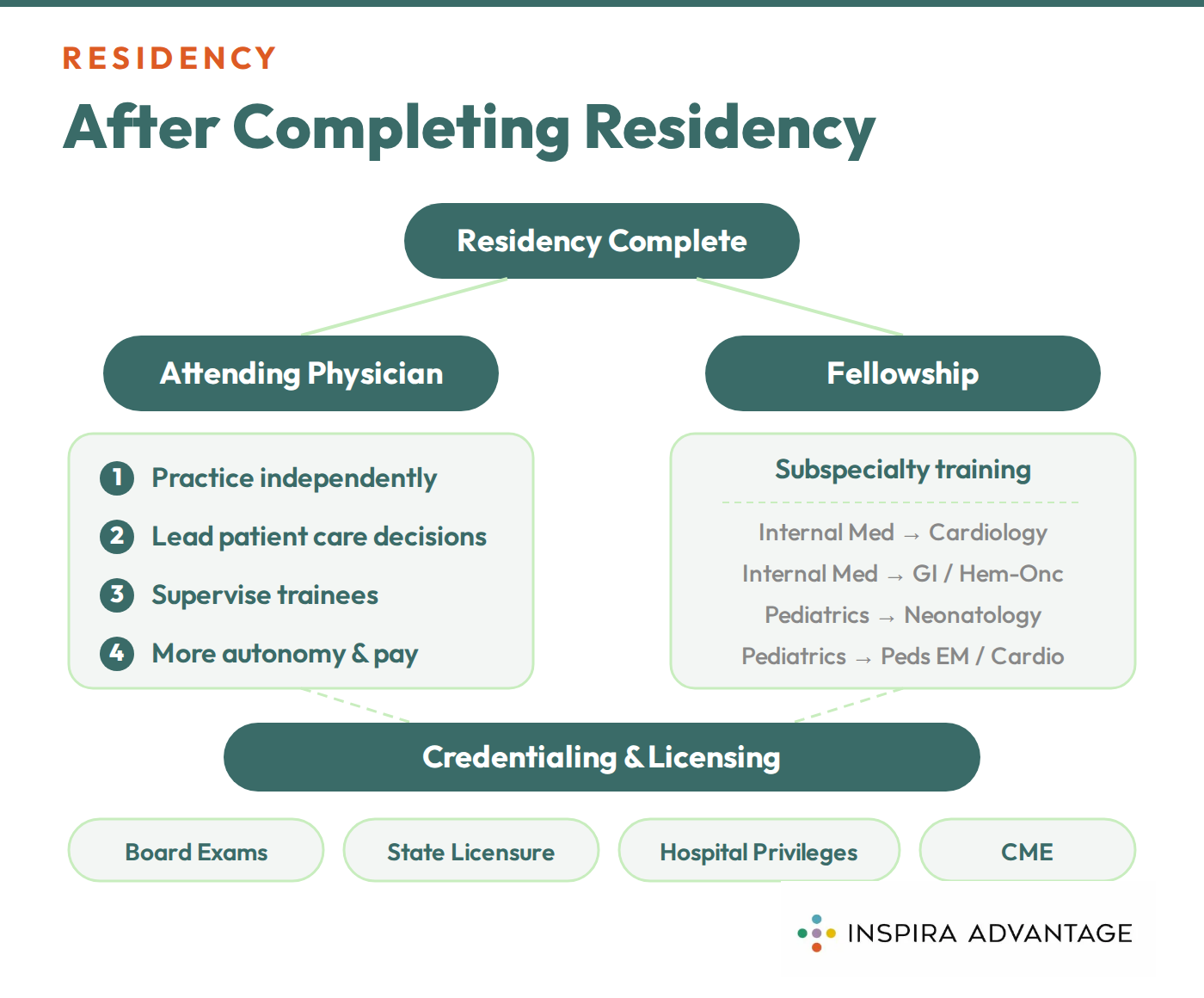
Some physicians begin working right away in hospitals, clinics, private practices, academic medical centers, or community health settings. Others pursue a fellowship to gain advanced training in a subspecialty.
For example, an internal medicine resident may complete a fellowship in cardiology, gastroenterology, or hematology-oncology, while a pediatrics resident may pursue neonatology, pediatric emergency medicine, or pediatric cardiology.
After residency, physicians also work toward meeting any remaining licensing, board certification, and credentialing requirements. This may include:
These steps help confirm a physician’s qualifications to practice independently in their specialty.
The transition from resident to attending often brings more autonomy, higher pay, and greater responsibility. For many physicians, this is the point at which years of medical school and residency training culminate in independent practice.
Residency in medicine refers to the supervised training that doctors complete after medical school to become qualified in a specific specialty. During residency, physicians care for patients in hospitals, clinics, and other clinical settings while working under the guidance of attending physicians. Residency usually lasts three to seven years, depending on the specialty. It’s the stage where doctors move from medical school knowledge to hands-on, specialty-specific practice.
Medical residency matching works by pairing applicants and residency programs through a ranking system. After applying and interviewing, applicants rank their preferred programs, and programs rank the applicants they want to train. A matching algorithm then uses both rank lists to place applicants into programs. Most U.S. medical students participate in the National Resident Matching Program (NRMP), commonly known as the Match.
Yes, residents are doctors who have graduated from medical school and earned an MD or DO degree. They are not medical students, but they are still completing supervised specialty training. Residents can examine patients, write orders, prescribe medications, assist with procedures, and help manage treatment plans. However, they still work under attending physicians until they complete residency and can practice independently.
Yes, residents can perform surgery, especially if they’re training in a surgical specialty. Surgical residents gradually build operative skills by assisting with procedures, performing parts of surgeries, and eventually taking on more complex responsibilities under supervision. The level of involvement depends on the resident’s specialty, year of training, skill level, and the attending surgeon’s judgment. Residents in non-surgical specialties may also perform procedures. But they typically don’t complete major operations.
No, not all hospitals have residents. Residents usually train at teaching hospitals, academic medical centers, and community hospitals affiliated with residency programs. Some hospitals focus only on patient care and do not operate graduate medical education programs. If a hospital has residents, a team that includes interns, residents, fellows, and attending physicians may care for patients.
Medical residency admissions can be very competitive, but the level of competitiveness varies widely by specialty and program. Fields like family medicine, pediatrics, and internal medicine are generally less competitive than specialties like dermatology, orthopedic surgery, plastic surgery, and neurosurgery. Applicants are evaluated based on clinical performance, board scores, letters of recommendation, research, specialty fit, interviews, and professionalism. Even in less competitive specialties, strong programs can still be selective.
Yes, medical residents can switch specialties during training, but it can be difficult and is not guaranteed. Switching usually requires finding an open position, getting support from the current program, explaining the reason for the change, and applying or re-entering the Match. Some completed training time may transfer, but residents often need to repeat part of the training if the new specialty has different requirements. Residents considering a switch should speak with program leadership and mentors early.
The exams required before starting medical residency usually include the USMLE or COMLEX, depending on whether the applicant is an MD or DO student. Most MD students take USMLE Step 1 and Step 2 CK before residency, while most DO students take COMLEX Level 1 and Level 2. Some programs may also consider additional exams, especially for international medical graduates. Exact requirements vary by specialty, program, and applicant background.




.svg)


